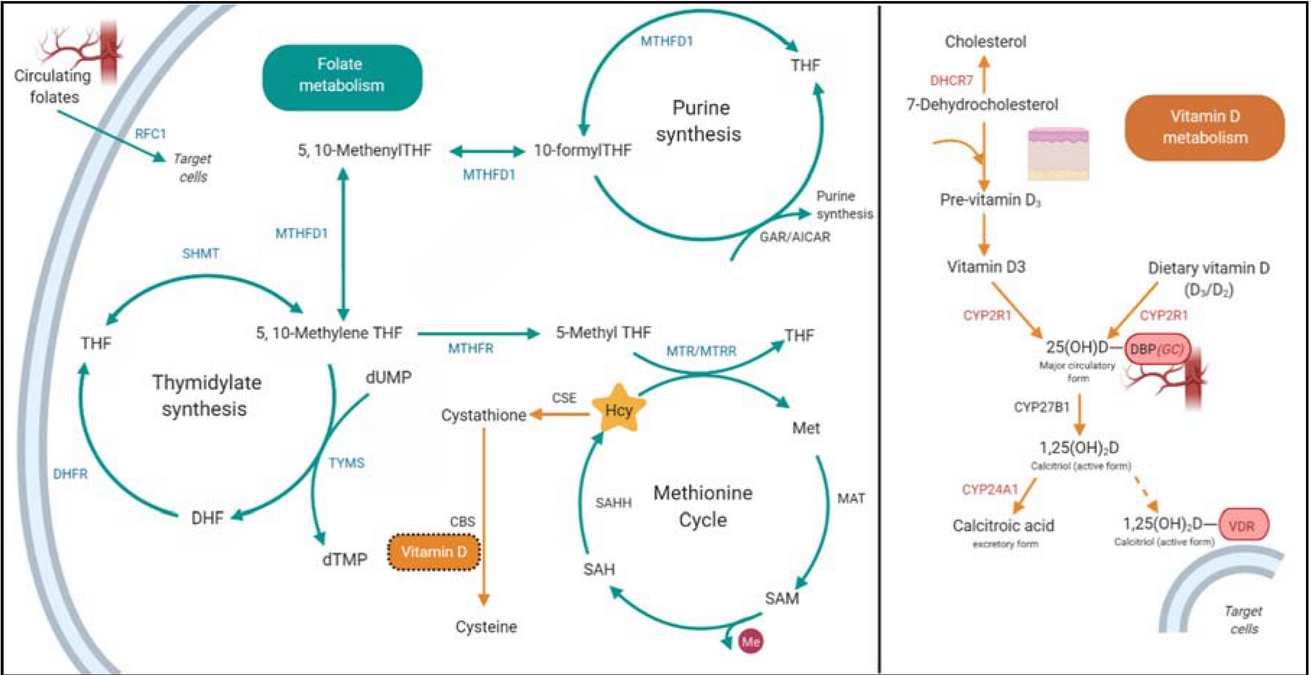
This test analyzes genes that affect the absorption of folic acid (vitamin B9) and its conversion to the active form (5-MTHF). It helps to identify congenital disorders that prevent the body from properly using folate, even with sufficient intake from food.
What genes are being tested?
- MTHFR (C677T and A1298C) — most important:
- Mutation C677T reduces the activity of the enzyme by 70%, which leads to the accumulation of homocysteine.
- A1298C causes less severe disorders.
- MTR and MTRR -affect the remethylation of homocysteine.
- DHFR -responsible for folic acid recovery.
Why do I need this test?
- Risk assessment:
- Thrombosis (due to increased homocysteine).
- Pregnancy complications (miscarriages, neural tube defects in the fetus).
- Depression, dementia (impaired neurotransmitter synthesis).
- Anemia (megaloblastic due to hematopoietic defects).
- Personalization of treatment:
- Selection of the folate form (regular folic acid may not be absorbed with MTHFR mutations).
- Dosage of vitamins B12, B6 and B9 to reduce homocysteine.
Symptoms of folate deficiency
They occur due to a violation of DNA synthesis and an excess of homocysteine:
- General information: weakness, pallor, dizziness.
- Neurological: irritability, depression, cognitive impairment.
- Hematological: megaloblastic anemia (large immature red blood cells).
- Pregnancy: malformations of the fetus (spina bifida, anencephaly).
- Cardiovascular diseases: early atherosclerosis, thrombosis.
Risk groups:
- People with a family history of thrombosis or miscarriage.
- Vegans (B12 deficiency worsens folate deficiency).
- Patients with autoimmune diseases (celiac disease, Crohn’s disease).
Symptoms of excess folate
Rare, but possible with an overdose of synthetic folic acid:
- Masking B12 deficiency (folic acid ‘corrects’ anemia, but does not stop nerve damage).
- Allergic reactions (skin rash, itching).
- Increased excitability of the central nervous system (insomnia, irritability).
- Growth of tumors (theoretical risk for pre-existing neoplasms).
Blood folate levels
Analysis for folate is performed in serum or red blood cells (a more accurate indicator).
| Parameter | Standard |
|---|---|
| Serum Folate | 7-45 nmol / l (3-20 ng / ml) |
| Folate in red blood cells | 360-1400 nmol / l (160-620 ng / ml) |
| Homocysteine | <15 micromol/l (optimal <8) |
For MTHFR mutations:
- Folate levels may be normal, but homocysteine levels are elevated (>10-15 mmol / l).
- Red blood cell folate is a more reliable marker than serum folate.
What should I do if mutations are detected?
- Replace folic acid with methylated forms:
- 5-MTHF (methylfolate) — is absorbed even with the MTHFR mutation.
- Dosage: 400-1000 mcg / day (for pregnancy up to 5 mg).
- Combine with vitamins B12 and B6:
- B12 (methylcobalamin) – 500-1000 mcg / day.
- B6 (pyridoxal-5-phosphate) – 25-50 mg / day.
- Control homocysteine:
- Target level: <7-8 mmol/l.
- Diet:
- Leafy greens (spinach, arugula).
- Liver, eggs, and legumes.
- Avocado, citrus fruits.
Example of a genetic report
Conclusion
- A genetic test reveals the risk of folate metabolism disorders leading to increased homocysteine.
- The deficiency is manifested by anemia, neurological and obstetric complications.
- Excess is possible only when taking synthetic forms.
- Folate norms: 7-45 nmol/l in serum, homocysteine <8 mmol/l.
- Treatment: methylfolate + B12 + B6 under the control of assays.
The test is especially important for those planning pregnancy and patients with a history of thrombosis.
Добавить комментарий